Recurrent Umbilical Hernia After Gynecological Surgery: A Case Report
A case report of a recurrent, incarcerated umbilical hernia in a 60-year-old woman with prior gynecological surgery - presentation, imaging, urgent surgical management, and the case for mesh repair.
Auste Treska, MD
Doctor of Medicine - medical writer & clinical researcher
Abstract
This case report details the treatment of an umbilical hernia in a woman who had previously undergone gynecological surgery. The patient, a 60-year-old woman, sought out medical attention because she was experiencing nausea and lower abdominal pain. She had gynecological surgery for uterine cancer in 2017, which included an umbilical hernia repair - but subsequently, the hernia recurred. This case highlights the clinical challenges brought on by postoperative incarceration and recurrent umbilical hernias. With a timely diagnosis and surgical intervention, positive outcomes can be achieved.
Introduction
Umbilical hernias are a common surgical problem (the second most common hernia in adults). These hernias can happen at any stage of life and often present as a noticeable bulge or swelling close to the navel, frequently causing discomfort and pain.
Reopening of a previously closed umbilical ring or surrounding tissue is the etiology of umbilical hernias. While tenderness and incarceration are typical physical findings, pain and gastrointestinal discomfort are also potential but uncommon symptoms (1).
Small umbilical hernias are frequently asymptomatic and rarely painful. Large umbilical hernias in older, multiparous, or obese women are usually symptomatic and usually manifest as a hernia that grows larger over time before becoming tender or irreducible in most cases. A common side effect of umbilical hernias is strangulation, which often manifests as a sensitive umbilical bulge, skin colour changes, and indications of intestinal obstruction (2).
An umbilical hernia is diagnosed during the physical examination. It is necessary to carefully examine the entire abdominal wall, particularly the area around the previous scar. It is possible to assess the hernia's size and content. To assess for problems, or if the clinical diagnosis is challenging - especially in patients with obesity - imaging investigations such as abdominal ultrasound or CT scan may occasionally be warranted. Given the elevated risk in certain patient populations, it is especially crucial to investigate BMI, smoking status, and any prior cirrhosis (2).
Although surgical intervention is frequently used to treat primary umbilical hernias, the recurrence of such hernias following first correction continues to pose a difficult clinical situation. The risk of incarceration and strangulation is increased by the typical small neck of umbilical hernias (2). The treatment of recurrent umbilical hernias has changed significantly over time, with mesh repair procedures being used more frequently. Because mesh repair has the potential to improve tissue reinforcement and lower the likelihood of hernia recurrence, it has become an important strategy in treating these recurrent hernias. It has benefits like increased repair strength and durability as well as a reduced likelihood of complications (3).
The patient, a 60-year-old female with a history of gynecological surgery, was diagnosed with a recurrent umbilical hernia causing lower abdominal pain and nausea, which emphasizes the significance of prompt diagnosis and efficient surgical management.
Patient description
The patient is a 60-year-old woman who presented with pain below the umbilicus, nausea, and vomiting once.
Case history
In 2017, the patient underwent a hysterectomy for cervical cancer. At the time of this operation, an operation for an umbilical hernia was also performed. There were no other prior surgeries performed. After some time, the hernia recurred.
Physical examination
Upon physical examination, the patient's general condition was satisfactory. Body temperature was 36.6 °C. The skin, mucous membranes, tongue, sclera, and heart activity were normal. Blood pressure was 174/81. BMI and the patient's height are unknown. Vesicular respirations were noted. The abdominal pain was rated 7 out of 10 by the patient. The abdomen was soft and somewhat swollen, with painful palpation on the right side. The hernia was painful and measured 8 × 5 cm. Peristalsis was present.
Investigations
Laboratory. Findings included elevated glucose (8.04 mmol/L), elevated neutrophils (85.2%), decreased lymphocytes (10.9%), decreased eosinophils (0.0%), elevated erythrocytes (5.51 ×10¹²/L), elevated hematocrit (0.471 L/L), and elevated CRP (9.98 mg/L).
Abdominal X-ray. No radiological signs of free air or bowel obstruction were seen. The lumen of the intestine was not significantly dilated; single liquid–air surfaces were noted in the intestines - one in the central/lower part with the proximal differentiated segment showing extinct haustration. Colitis was suspected because of changes in a short segment of the intestine.
Abdominal ultrasound. Findings were consistent with a stuck (incarcerated) hernia - collapsed loops of small intestine without registered peristalsis and free fluid in the hernia sac (large sac; the gate was not clearly visualized).
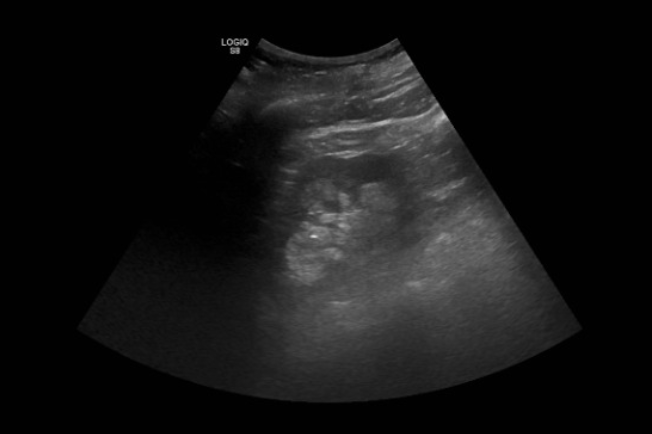
Figure 1. Abdominal ultrasound - incarcerated hernia: collapsed small-bowel loops without peristalsis and free fluid within the sac.
CT angiography (urgent, IV contrast, no oral contrast). Findings: anterior abdominal-wall hernia, gate 30 × 28 mm, sac 97 × 85 × 67 mm, contents of an ileal loop, walls contrasted and flaky, traces of fluid in the sac, tissue infiltration - consistent with a stuck hernia; signs of ileal obstruction. The main vascular trunks of the abdomen were contrast-enhanced with no signs of thrombosis in large veins; traces of fluid were noted in the pelvis.
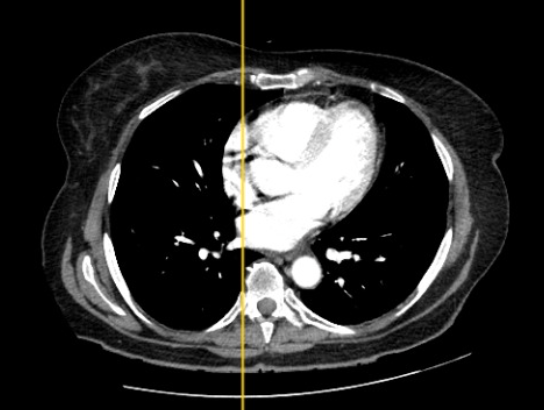
Figure 2. CT angiography (axial), with sagittal localizer line.

Figure 3. CT angiography (axial), abdomen - hernia sac containing an ileal loop with surrounding fluid.
Treatment plan
Urgent surgical treatment - hernioplasty (hernioplastica, adhesiolysis, resectio omenti majoris, sutura inversa) - was indicated. The plan included antibiotics (cefazolin 2 g IV), infusion therapy (Ringer's solution 1000 mL IV), and analgesics as needed.
Expected outcome
After the diagnosis, elective repair was suggested. Mesh reinforcement was not done but could have been advised, since suture repairs have a high probability of recurrence. Mesh can be inserted laparoscopically or openly with favorable clinical outcomes. While composite meshes must be used for laparoscopic repairs, standard polypropylene mesh is sufficient for open onlay techniques. Large seromas and surgical-site infections are rather frequent side effects that can cause recurrence (3).
Actual outcome
A 15 cm longitudinal incision was made bypassing the umbilicus from the left. A 12 × 8 cm sac of an incarcerated subumbilical hernia was identified; the surrounding tissues were bluish, and when the sac was opened, a cloudy hemorrhagic fluid came out. After resection of the changed tissue and release of the constriction, the strangulation furrows of the small-intestine wall disappeared within 5 minutes, leaving only blood imbibition of the affected intestine and hyperemia of the wall. Lidocaine was injected and the affected intestine was covered with a 0.9% NaCl bandage.
After another 15 minutes, intestinal peristalsis was restored and the hyperemia of the sac and wall decreased. In several places, the wall of the small intestine was closed with single 3-0 PDS sutures in the areas of former strangulation furrows. The abdominal cavity was drained and the intestine was returned to the abdominal cavity. The aponeurosis (8 × 4 cm defect) was sutured with single 2-0 and continuous 1-0 PDS sutures. The skin was washed with betadine, the navel was fixed, and the skin was closed with sutures before a bandage was applied.
The patient's final diagnosis was hernia tegmenti abdominis postoperativa incarcerata, M3L1. The patient's condition after surgery was satisfactory: the abdomen was soft, painless, and without peritonitis; peristalsis was heard; and the surgical wound healed normally, without signs of infection or infiltration.
Discussion
The main objective of umbilical hernia repair is to create a long-lasting closure of the abdominal fascia while reducing discomfort and the risk of complications like surgical-site occurrence (SSO), intestinal injury, early or late infections, and hernia recurrence. Numerous surgical procedures have been discussed, including simple suture repair, open repair with mesh, open repair with prefabricated mesh "patches," laparoscopic repair, and even robotic repair (4).
Mesh repair for umbilical hernias larger than 3 cm has become more common in recent years, because mesh repair has a lower recurrence rate than open suture repair (1). Mesh reinforcement seeks to correct any structural flaws that may have led to the initial hernia formation. For umbilical-hernia defects under 2 cm, suture repair is frequently utilized; but when defects are over 4 cm, this approach has been linked to recurrence rates of up to 54% (5).
Both open and laparoscopic techniques can be used to implant meshes. In general, surgeons favor the method they are most experienced with or follow their patients' choices. The simplest method - placing an open onlay mesh - needs subcutaneous dissection, which in some situations might result in seroma or hematoma followed by surgical-site infection. Mesh may also be positioned sublay or preperitoneally; while avoiding significant subcutaneous dissection, reducing seroma production, and potentially reducing recurrence, this may need more surgical experience and ability. In complex or recurrent cases, the implantation of onlay and sublay mesh can be done simultaneously to offer a more durable repair (3).
The most-used prosthetic material, particularly for open onlay repairs, is standard polypropylene mesh; thin macroporous meshes are also in use. Both kinds are appropriate for use as onlays and sublays. Creating a "lightweight" mesh by lowering the density of polypropylene reduces the foreign-body reaction, improves abdominal-wall compliance, lessens mesh contraction or shrinking, and promotes better tissue incorporation (6).
Recurrence following umbilical hernia surgery has been attributed to a number of causes. Classic contributors include a large seroma and infection at the surgical site. Obesity and rapid weight gain after surgery are risk factors; a BMI > 30 kg/m² and defects > 2 cm could contribute to surgical failure, and smoking may affect recurrence as well (7). Surgery should not be delayed, as a higher incidence of complications can occur: surgery postponed by more than one day has been linked to a higher rate of significant complications, a longer average postoperative stay, a higher risk of repeat surgery, a higher risk of readmission, and a higher risk of death within 30 days (8).
Conclusions
This case report highlights the importance of considering mesh repair methods for recurrent umbilical hernias, especially in patients who have had prior gynecological surgery. Early identification and effective surgical therapy are the keys to attaining positive clinical results and lowering the risk of complications. To improve patient care in these situations, further study and consensus on the optimal method for umbilical hernia repair are required.
In this instance, a 60-year-old woman who had previously undergone gynecological surgery was diagnosed with a recurrent umbilical hernia after presenting with lower-abdominal pain and nausea. The treatment strategy included hernioplasty in addition to antibiotic medication and infusion therapy, because urgent surgical intervention was determined to be required. The outcome of the procedure was successful and the patient showed no indications of infection or complications during or after surgery. Given that mesh reinforcement dramatically lowers the risk of recurrence compared to open suture repair, this example emphasizes the value of mesh reinforcement in hernia surgery, especially for hernias larger than 3 cm.
References
- Maia, R. A., Salgaonkar, H. P., Lomanto, D., & Loo, L. Umbilical hernia: when and how. AME Publishing Company; 2019. https://ales.amegroups.com/article/view/5123/html
- Coste, A. H., Parmely, J. D., & Jaafar, S. Umbilical hernia. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK459312/
- Kulaçoğlu, H. Current options in umbilical hernia repair in adult patients. https://pubmed.ncbi.nlm.nih.gov/26504420/
- Moradian, S., Klosowiak, J. L., Dumanian, G. A., Park, S., Issa, T., & Boctor, M. J. Novel approach for umbilical hernia repair using mesh strips. Plastic and Reconstructive Surgery – Global Open. http://dx.doi.org/10.1097/gox.0000000000004947
- Madsen, L. J., Oma, E., Jorgensen, L. N., & Jensen, K. K. Mesh versus suture in elective repair of umbilical hernia: systematic review and meta-analysis. 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7260408/
- Cobb, W. S., Heniford, B. T., & Kercher, K. W. The argument for lightweight polypropylene mesh in hernia repair. https://pubmed.ncbi.nlm.nih.gov/15846448/
- Venclauskas, L., Silanskaite, J., & Kiudelis, M. Umbilical hernia: factors indicative of recurrence. https://pubmed.ncbi.nlm.nih.gov/19124962/
- Leeds, I. L., Jones, C., DiBrito, S. R., Sakran, J. V., Haut, E. R., & Kent, A. J. Delay in emergency hernia surgery is associated with worse outcomes. 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8710144/